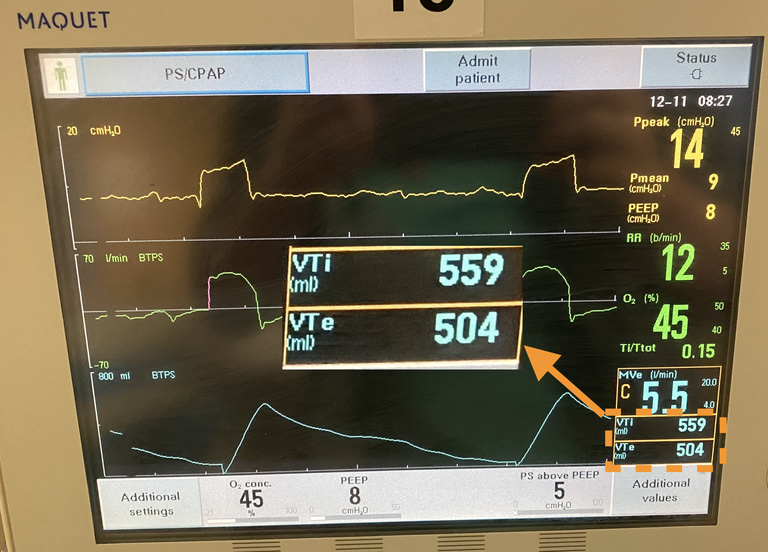
The tidal volume is the volume of air moving in and out of the lungs with each breath. Approximate average values in normal conditions are ~500 mL for an average healthy male and ~400 mL for an average healthy female. Too much tidal volume can result in over-distended lungs, and lead to barotrauma.
To the left is the tidal volume displayed on a Maquet ventilator. Here tidal volume inhaled (VTi) and tidal volume exhaled (VTe) are given; the lower value of VTe is due to bleed-off in the circuit.
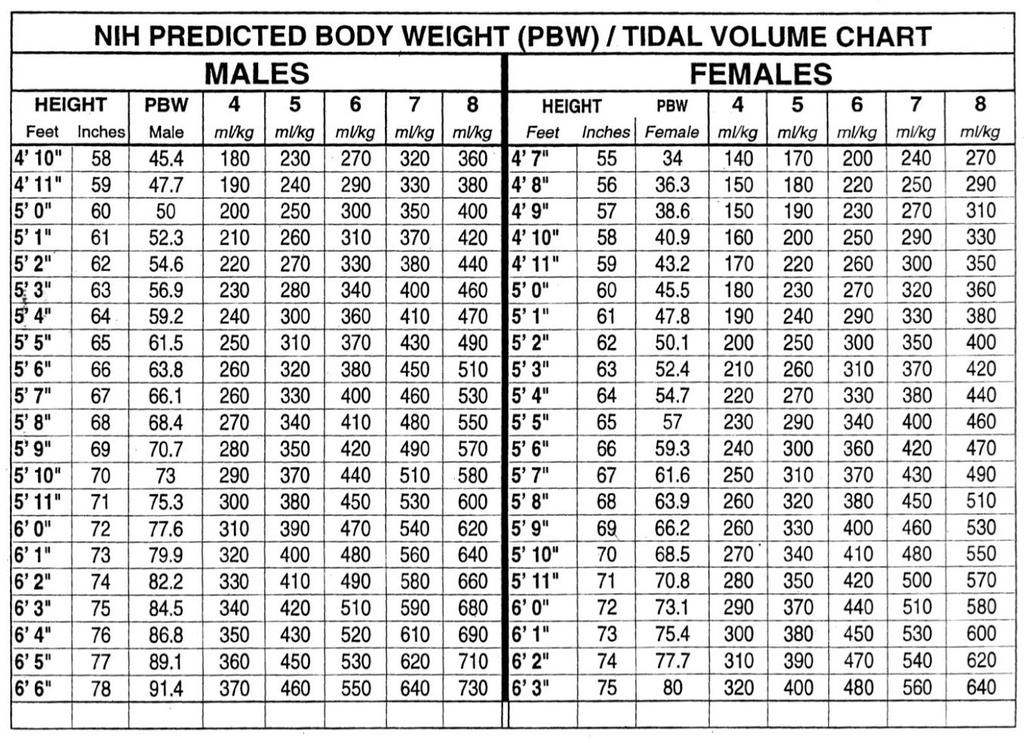
To calculate an initial tidal volume on the ventilator, the ideal body weight is often used. A person’s ideal body weight is calculated based on their height and gender: it reflects the fact that lung volumes will vary depending on height and gender, but not necessarily with actual weight (i.e., an overweight or obese person does not gain lung volume as they gain weight).
Once the ideal body weight is known, the tidal volume can be calculated; typical starting values are 6 to 8 mL/kg of tidal volume per kg of ideal body weight. In lung-protective ventilation strategies used in ARDS, 6 mL/kg is often used as a goal tidal volume
To the right is the ARDSnet table for calculating tidal volumes. For a given height in each gender, a predicted body weight (PBW) is given with corresponding tidal volumes: for a 6 foot tall male ventilated at 6 mL/kg the tidal volume would be 77.6 kg (the PBW) x 6 mL/kg = 470 mL.
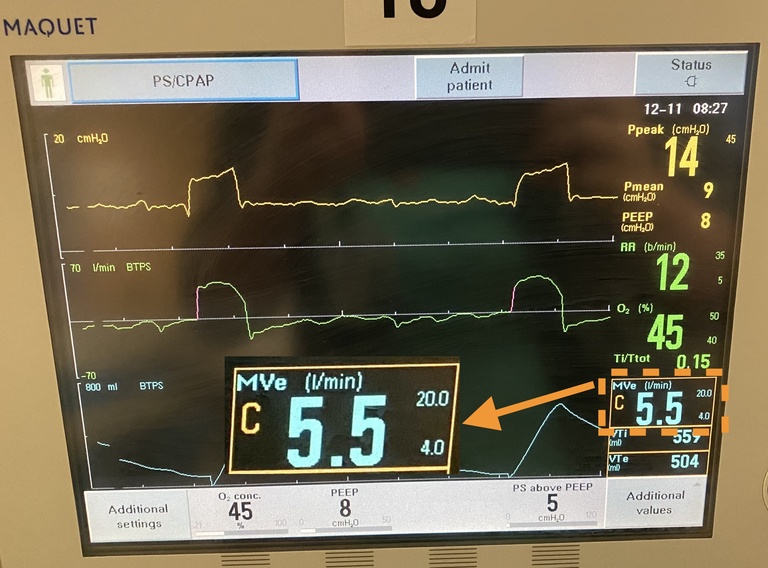
and expressed in terms of liters per minute
A related concept is the minute volume (MV), equivalent to the product of the respiratory rate (RR) and tidal volume (TV) (RR x TV = MV). A typical minute volume for a healthy adult is 70-110 ml/kg/min. Goal minute volumes can be reached by changing the respiratory rate or the tidal volume. In the above-mentioned example of ARDS (or other instances where the lung is poorly compliant), lower tidal volumes are used to prevent over-distension and barotrauma; this is compensated by higher respiratory rates to produce a stable minute volume (for ARDS respiratory rates of 18-22 are often used). In cases of acute asthma, as previously mentioned in the Respiratory Rate section, the respiratory rate often has to be lower to give sufficient time for expiration to complete; thus, an increased tidal volume can be used to maintain an appropriate minute volume.